



The maelstrom around drug pricing has continued its fury over the past month, which has led to considerable volatility in the biopharma stock market. Investor fears of draconian price controls that will eliminate the return of investment from innovative pharmaceutical R&D are almost certainly overblown, but they do create a lot of market anxiety.
The current widely-held assumption on the part of the investment community is that any pressure on pricing is a wholesale bad for our sector. It certainly is a challenge for those reliant on large semi-annual price increases for their revenue growth, which includes many of the largest biopharma companies; without these price increases, sales figures would sag, analysts would downgrade, and stock performance would suffer.
A downdraft in large cap biopharma revenues, followed by generalist investor malaise about the industry as a whole, would certainly drive away some of the capital in the space. Indeed, we’ve already seen the macro impact of negative pricing sentiment on fund flows: of the $16B in capital that flowed into the sector between 2013-2015, about half of it has flowed out in 2016, according to data from Raymond James. These negative fund flows are a drag on stock performance, as sellers outnumber buyers in both individual names and indirectly in the broader ETFs. These pressures makes it hard for investors to be excited about putting more capital to work in aspiring IPOs, which tightens up the pool of mezzanine crossover capital used to scale the next crop of public biotechs.
Fear and greed cycles are endemic in capital-hungry sectors. Right now, and since last summer, we’ve clearly been in a fear part of the capital cycle. If the current negative sentiments and pricing fears scare away more of the much-needed growth capitalbad thing for our R&D-heavy sector; it’s hard to build young biotech companies without access to equity capital, as the revenues required to self-fund are off in the distant future for most of them.
So if pricing pressure in our sector causes a sustained pullback from public and late stage investors, there’s little to prevent the downward push from working its way upstream and damaging the early stage biotech community. Or is there?
At the risk of wearing brightly rose-tinted glasses, I actually think there’s a reasonable and positive countervailing force that could continue to support very strong investment performance for early stage suppliers of innovative new medicines, like those in the VC-backed biotech subsector.
Here’s the alternative thesis:
Revenue quality and growth are a big part of large cap biopharma story today, and those with higher revenue growth rates have better trading multiples and valuations, as you might expect. With patent expiry on major products, even treading water with revenues is a feat for some large cap names. EPS is certainly a related and important variable in the large cap story, but it’s one easily manipulated through stock buybacks and short-term executive incentives, as Jeremy Levin recently articulated in BioCentury (here). But at the end of the day, driving revenue is critically important in the large cap universe, perhaps even existential.
Revenue is obviously a function of both price and volume. As many have highlighted, and is particularly well captured in IMS’s recent Health Affairs article, the bulk of pharmaceutical revenue growth over the past decade has come price increases of established branded products. The large cap biopharma industry’s equity performance has largely been supported by price increases in the US market. But times are changing.
The era of bi-annual, double-digit price increases of many established branded products is almost certainly coming to an end, given the renewed fury and emerging self-regulating sentiment; instead, prices of established branded drugs, in general, are much more likely to trend only modestly higher than inflation (mid-single digits). Further, after Mylan’s EpiPen fiasco, there appears to be a broad industry support for drawing a clear distinction between Innovators vs Exploiters, and pushing forward with initiatives opening up more generic and price competition, list-to-net price transparency, and the like (see Forbes post from several high profile CEOs here). In an impressive sign of industry leadership and self-regulation, Brent Saunders, CEO of Allergan, has announced a pricing pledge to limit increases to “no more than once per year and, when we do, they will be limited to single-digit percentage increases.” Other companies appear posied to follow suite. Hillary Clinton has recently put forward a plan targeting “unjustified” price increases, and Donald Trump has wailed on the pharma industry.
All this conspires to reinforce the belief that price increases of established products aren’t going to drive revenue in the next decade the way they have in the past one. This means future revenue growth has to be made up by volume.
But volume is essentially prescription growth – more patients taking their medicines – and this hasn’t been a big lever. Most established incumbent brands haven’t witnessed significant (or any) volume growth over the past five years; in fact, many of them are negative or flat. As highlighted in the WSJ a year ago, 50% of the top 30 pharmaceuticals saw less than 5% volume growth between 2010 and 2014, and twelve of those actually saw volume losses. While the biggest downward force on overall pharma industry spending was the loss of exclusivity of other branded products, the aggregate reductions in prescription volumes for incumbent products (those with more than two years of sales) has been the second most significant constraining force (see Exhibit 2 of this Health Affairs paper). So despite lots of marketing spend, including DTC ads, the aggregate impact on prescription volume for incumbent branded drugs was collectively negative. There are certainly many brands with huge volume growth, like Revlimid, Humira, and Stelara, but in aggregate mid- and late- lifecycle prescription volume growth has not been a huge driver of revenues.
So the only way to drive portfolio product volume is to launch more, and, importantly, more innovative products. New products that are priced at a premium because they are cost-effective relative to the benefits they deliver. Like Sovaldi, or Keytruda and Opdivo, where the price is justified by the magnitude of the medical benefit.
But how will Pharma do this?
R&D productivity inside of big bureaucratic organizations remains challenging; and, even though glimmers of hope are being seen, it’s hugely costly, and complex, to bring a drug from idea to market inside of a large company. Further, in order to compete, established brands require extensive post-market clinical trials and Phase IV activities, which consume 30-40% of most big biopharma R&D budgets. Lastly, and a related point, R&D budgets have been and continue to be under fire across the industry, with typically fewer relative dollars channeled into in-house drug discovery and early research than in the past. In short, the only way for big biopharma to launch more products is to aggressively source more of their pipeline externally. By some estimates, externally-originated assets are already ~50% of many large cap pipelines; in the future, it’s likely even more.
More aggressive deal-making means that assets delivering significant medical impacts – or those offering the real promise of doing so – will be even more sought after in this new market dynamic than they are today. Over the past few years we’ve already seen upticks in both R&D-stage M&A and licensing activity. The relative scarcity of truly innovative assets, and the fear of being boxed out of access to them, will increasingly drive big biopharma BD&L activities both for late stage programs (where there’s a paucity of unpartnered assets as it is right now) and early stage collaborations. Think about some of the big M&A deals of late: Medivation-Pfizer, Onyx-Amgen, Receptos-Celgene, and StemCentryx-AbbVie. While the former two have sales, the latter two were around mid- and late-stage assets. We’ve benefited recently from the increased appetite for early stage, innovative assets with Padlock-BMS and Nimbus-Gilead. Further, it’s very likely that strategic deal-making, akin to the BMS “String of Pearls” and “Celgene-model”, will spread wider across the industry in order to build broad, distributed portfolios of external assets with fractional or option-based ownership rights. These and other external R&D tools will amplify their roles as strategic differentiators and force multipliers for R&D.
While public market investor demand for emerging biopharma often cycles with sector fund flows, it’s worth highlighting that the demand from “big” biopharma dwarfs it, even at the peak of most cycles. Since 2013, biotech IPOs have raised nearly $15B from public investors, with aggregate market valuation of $56B at offering (for ~150+ IPOs). In the same period, $100B of R&D-stage biopharma M&A (private and public) has been announced, along with $21B in upfront licensing payments (and a further $185B in contingent “biobucks”). There are more than 50 global pharma companies with greater than $2B in sales – that’s a lot of potential buyers/partners looking to access new products to strengthen future revenues.
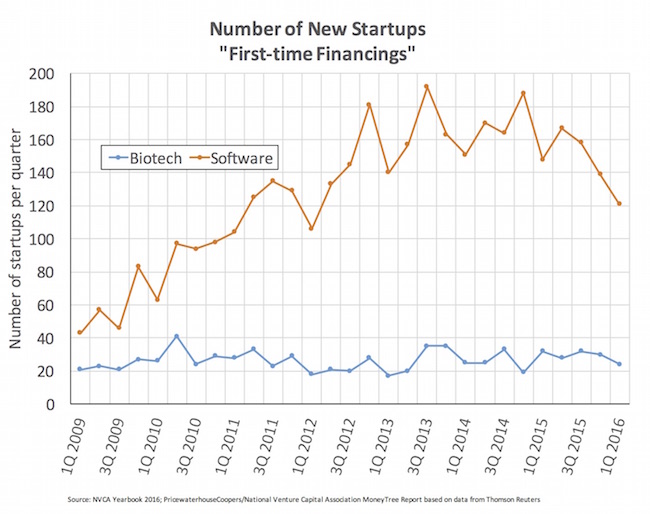
Further, there’s a real scarcity to the supply of innovation able to feed this volume-required demand. The number of new biotech startups each quarter remains largely flat since 2009, as described here many times, and the constrained supply dynamic is likely to persist. There are also relatively few investment firms focused on creating and launching of the next wave of new biotechs, a dynamic that is also unlikely to change, especially if broader investor malaise around the publicly traded biopharma stocks continue.
{kind=link}
So in summary – given the dynamics around pharmaceutical pricing and volume in our industry, it seems very likely that the demand for innovative products and pipeline will accelerate in the coming years in order to support the revenue needs of larger commercial-stage companies. Those needs won’t be met in the future by aggressive price increases: only through the launches of a greater number of innovative medicines will prescription volume contribute to aggregate revenue growth. This new product demand can’t be met through internal R&D on its own, even with the current external:internal mix. Therefore, startup and emerging biotech is uniquely positioned as an even greater future supplier of innovation to the larger players, and this will translate into a tailwind for returns to the early stage investors that back the winners among them.
This alternative thesis isn’t on the minds of many investors, especially those with short-term fears of politically-inspired price reductions. But as a long-term investor, you have to look at how these broader macro forces are shaping our industry’s structure – which is why we and otehrs remain bullish on the prospects for early stage biotech investing.