



The perennial drug pricing debate has reached a fever pitch, as loud as it’s ever been over the past few decades. Politicians on both sides are bashing the drug industry with the typical talking points about exorbitant prices, countered of course by the expected talking points about innovation and impact from PhRMA and BIO. Even VC’s and biotech CEOs are actively engaged in letter-writing campaigns to support the industry.
This week Congress is considering a piece of proposed legislation, known as “The Lower Drug Costs Now Act” (or H.R.3), which is similar in form to many of the proposals from multiple presidential candidates (like Elizabeth Warren). Let there be no mistake: these proposals would fundamentally damage the landscape for biomedical innovation in the US.
Even the CBO models that these proposals would lead to a significant reduction in the development of new medicines. This is a very bad outcome for both society and the biopharma sector. I truly hope rational minds will prevail when the legislative process concludes.
Questions have been raised about whether these new pricing proposals will negatively affect early stage biotech venture capital flows and the behavior of the investment community (from causing a “nuclear winter” to those asking “well where else will VCs invest”). The answer is simple: of course they will affect investment.
As a front-line practitioner in early stage biotech venture capital, I can assure you that radical across-the-board cuts in the future pricing of innovative therapies will certainly affect both the scale and pace of investments in new biomedical startups.
I’d like to share my perspective in three sections. First, I’d like to frame some foundational assumptions about investing in new therapies and the implications of radical pricing changes. Second, before we can talk about solutions, we need to share a common understanding of the state of healthcare and how pharmaceuticals fit in. And lastly, I’ll close with my thoughts on a few real measures for pricing reform that make sense. Although far too many words, a nuanced topic like drug pricing needs context – so there’s plenty of it for those willing to read on.
First Principle
Over the last fifteen years, I’ve invested with one foundational assumption – a variant of the George Merck view that patients come before profits. It’s what I call the “first principle” of early stage biotech investing: if we can positively impact the lives of patients by discovering and developing an innovative new medicine, the system will reward that risk-taking with superlative investment returns.
We all know the talking points about biotech being long, costly, and risky: it takes an average of 15 years from idea to product, hundreds of millions of dollars in direct costs per program, and 90% of drugs fail before making it to market. These are the inconvenient truths of drug R&D, and I won’t go into them here.
But they markedly differentiate new therapeutic ventures from most other areas of venture capital; because of this challenging triad of features, early stage biotech venture investors can typically only really underwrite a portion of the R&D value chain. Most of us never see real revenues during the time course of our investment. If a company got started from scratch in drug discovery, we generally never even see new product launches within our 5-10 year investment cycle. I can’t even recall ever building a spreadsheet model with revenues and drug prices in it for any of our new biotech investments. You simply can’t model with any accuracy what the revenues will look like in 15 years when a future drug launches. When we start a drug discovery company, the time to market is too long, the costs to get there too big, and the unpredictability too vast to build a model that is remotely useful. What we do know, with some accuracy, is what the real world unmet needs are for patients, and how we might address their mortality or morbidity. Our new startup investment theses are usually framed purely with that in mind.
In line with that approach, venture investors like Atlas can aptly be called “risk capitalists”. We underwrite lots of different kinds of risk. Foremost is the science risk – making medicines is incredibly hard, as biology and chemistry are way more complicated than textbooks tell you. But there’s also team risk, execution risk, financing risk, competitive risk, etc… And we take on these risks over 5-10 year investment horizons.
Importantly, once we are in a private biotech investment, we also face real “exit risk” as we have no real liquidity in our portfolio. That is, the only way we can leave an investment and recycle profits into new funds (and thus new investments) is by truly exiting it: selling the company to a bigger biopharma, offering a share of the company to the public markets and trading out over time, or writing it off/walking away. Unlike traditional public investors, who can move their capital from one investment to the next, one sector to another, or even into cash on the sidelines – we can’t do any of that once our capital is deployed. This creates significant illiquidity, another form of long duration exit risk. All this means we must have real conviction about what the long range future looks like and the expectation that we’ll be compensated for locking up our capital for a decade or more. In short, we have to have confidence in our expectation that the “first principle” of early stage biotech investing will be intact.
Underwriting all of these risks, and appreciating where we operate in the ecosystem, early stage VC-backed biotechs typically aim to advance new drugs from idea to clinical proof of concept, and then pass the baton to downstream partners through an IPO or M&A to take the new potential medicine (and company) the rest of the way. These downstream partners are larger biopharma players and/or later stage investors like hedge and mutual funds. Because these new partners join us midway through the R&D journey, they are much closer to any potential product launch and market dynamics. These are the folks who rightfully do build spreadsheets, as any smart later stage player should. They do run NPVs from discounted cash flows. They run product launch scenarios. They take bets on late stage clinical outcomes and approvals. And, importantly, they model what drug pricing is likely to be.
This is where the ripple effects of poorly conceived drug pricing legislation can become a tsunami of risk for early stage investors like me. If these downstream partners see their models come down by 70% (like Warren’s explicit proposal or implied by H.R.3), it will have a huge impact on how they invest in (or not) our early stage biotechs. Without the availability of downstream capital, we can’t keep advancing new medicines. Even successful biotech companies will often burn capital without real revenues for 15-20 years. This means biotech, as a sector, is very sensitive to the actual and perceived availability of capital. These new pricing measures will almost certainly tighten capital flows and dramatically increase the risk profile of our early stage investments (especially financing risk, exit risk, illiquidity risk, etc) way beyond the already prodigious science risks we take.
As these aggregate risks go up, the required rate of return goes up to compensate for heightened probability of investment losses. And this leads to a more expensive “cost of capital”. In plain English, that means venture money will become scarcer and more expensive to raise in light of the elevated risks. This is the painful world we’ve been in before (as two examples, take the challenging periods of 2002-2004 and 2008-2010): the venture money supply tightened dramatically in those periods, after peaking exuberantly shortly before. Funding flows in venture-backed biotech have been exuberant over the past few years, but a step-change in risk will dramatically tighten available funding for biotechs; when VCs become more risk averse, it means less innovative science will be able to find adequate funding.
In light of all of these dynamics, in order to continue to invest in turning risky science into new medicines, we need to have faith that the future healthcare system in the US will respect the “first principle” of early stage biotech investing: if we deliver real value to patients we will be rewarded with outsized returns. Sadly, the current pricing legislation being debated raises real questions for me about its fidelity.
But only asserting that the current drug pricing proposals violate this first principle isn’t very constructive: what are some possible solutions to the challenge of rewarding innovation while addressing the cost of pharmaceuticals?
In order to get to that, we need to have a shared sense of the situation.
Observations about the US Healthcare System and Pharmaceuticals
Here are a dozen or so points about the US healthcare system and pharmaceuticals that are important to appreciate before discussing pricing reform. Many of these are well known, but I’ll try flesh out the less well-appreciated points.
- Healthcare has historically been growing as a share of GDP for decades, though has plateaued around 17-18% recently. Overall healthcare spending is a concern for many, and it’s a worthy debate to discuss whether in an affluent society we should be spending 18% of GDP on our healthcare. But that’s a broader point and not the topic at hand.
- Pharmaceuticals haven’t grown as a share of healthcare spend. Drugs remain 9-10% of total healthcare spend for decades. Recent data suggests aggregate drug prices actually went down for the first time in 40+ years in 2018, due to generics and pricing restraint. Although there are a number of egregious examples of price increases (which I’ll address below), the reality is aggregate national pharmaceutical spending is just not a major driver of healthcare spending in the US – its less then 10 cents of every dollar.
- Consumers have increasingly been paying larger share via out of pocket spending. Changes to health insurance, with larger copays and deductables, and “donut holes” in coverage, have created significant out of pocket costs to consumers. Much has already been described about this issue, and it’s an important one. This isn’t sustainable and needs to be addressed, especially for expensive specialty drugs.
- Pharmaceuticals are a more consistently priced and efficient tool for health impact than other medical interventions. Unlike health provider services, pharmaceutical products generally don’t dramatically vary in either cost or outcome in the same significant way other healthcare services do across the country. For example, the costs to a health care plan for an angioplasty/PCI after a heart attack can vary by 500% even in the same metro geography, depending on which hospital does the surgery (here). This massive variation doesn’t happen at the pharmacy, but is seen across a vast number of healthcare services (more examples from the Kaiser Family Foundation). If you aren’t near a top academic medical center, you may not get a best-in-class surgery or treatment; but if you are near a pharmacy and have insurance, as the vast majority of Americans do, you will typically be able to get best-in-class medicines. Because of that, drugs have the potential to democratize healthcare. If drugs are truly effective and reduce visits, sickness, and system costs, there’s no reason prescription medicines shouldn’t actually be a higher proportion of healthcare costs vs far less efficient medical services.
- Unlike all other healthcare expenditures, pharmaceuticals commoditize rapidly once the products are beyond their patent-protected exclusivity period. The comparison of Lipitor in 2003 vs today is worth reviewing: in 2003, Lipitor was ~$3800/year for healthcare plans, today it’s about $50/year, over a 95%+ drop in cost. In contrast, laproscopic appendectomies, a very rote and common surgery, went from an average of $8.5K in 2003 to over $20K in 2016. Full knee replacement surgery from $19K to $34K, both according to the Kaiser Family Foundation. The reality is despite the maturity of the surgical technique, healthcare services don’t go generic – they actually get more expensive for most providers, and at a faster rate than inflation. This is yet another reason effective pharmaceuticals are a very cost-efficient long-term medical intervention; over longer time horizons, generic competition captures a huge amount of cost and delivers it as a dividend to society.
- Generics are a major boon to society and to the future innovators in the pharma industry. As noted above, the expiry of patents and the loss of market exclusivity herald a massive commoditization of prices for most pharmaceutical products. Genericization puts about 10-15% of total industry revenues at risk of significant price erosion in any given period, and has done so for several decades. This is what creates the room for new innovator products in healthcare budgets. Today, 90% of the ~6 billion monthly prescriptions written each year in the US are filled with generic drugs, all of which were at one time more expensive branded drugs. In healthcare, generics are the gift that keeps on giving – and a gift from the original innovator. But interchangeable, generic biologics haven’t yet happened despite a trickle of biosimilar approvals, even after 20 years of discussion. This has become a moral issue and affront to the industry’s social contract, especially when many of the older biologic drugs are taking double-digit price increases even after being on the market for 15+ years. These are, in my opinion, egregious drug pricing examples that need to be addressed.
- The US healthcare system is stacked against lower drug prices. Almost every player in the healthcare system is actually incentivized for higher drug costs (e.g., PBMs, physician practices, hospitals, distributors, etc) because they get paid a percentage of list price value, or get rebates off of those values, or mark them up when they pass the bill onto patients’ insurers. Most players in the healthcare value chain, whether they admit it or not, financially benefit from high-priced drugs: the higher, the better. This actually creates barriers to real price competition in crowded classes, as well as challenges for the adoption of lower cost drugs (like biosimilars) that might threaten those large rebates/discounts/mark-ups.
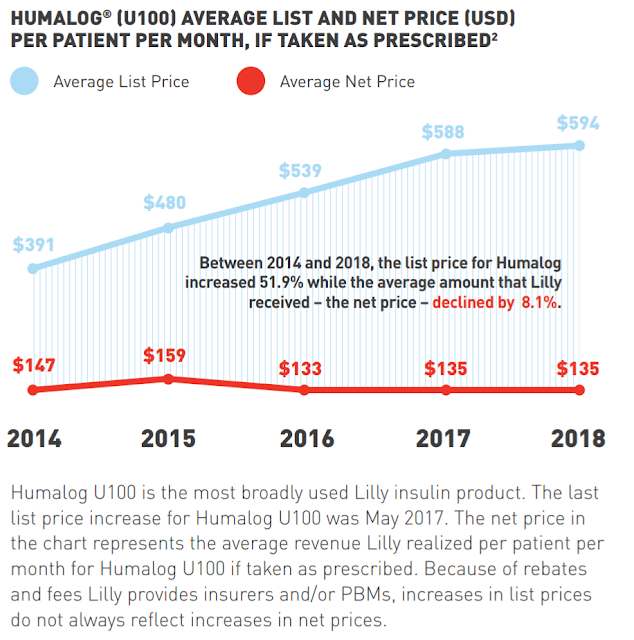
- List prices today do not transparently reflect pharmaceutical spending. The gross-to-net price differential distorts the market and has become a major issue. Pharmaceutical products have a list price for insurance companies, but this doesn’t reflect the value sent back to Pharma companies, as the system’s middleman extract their fees, rebates, and discounts. There is often a large (and lately increasing) delta between the list price of drugs and the net price back to the manufacturer. This has created a “gross-to-net bubble” that’s enormous, and is also enormously distorting to a discussion about drug prices. In the past few years, we have seen very small increases in net prices (1-2%). In fact, net prices increased only 0.3% in 2018, according to IQVIA; this is below the rate of consumer price inflation. As an example, branded insulin prices are commonly cited as having had egregious increases over time, and it’s true the list price increases have been very aggressive. But the net prices sent back to Pharma have often been very small if not negative. For a shocking image of this, check out the list-to-net price comparison of Humalog 100: $594 list price and a $135 net price after rebates. That captures the absurdity of the system. Adding insult to injury, that gross-to-net price differential isn’t passed on to consumers – it’s captured by the middleman usurpers in the healthcare system.
- Huge international price differentials exist for drugs across countries. It’s well appreciated that the US is paying more for most branded drugs, an average of 2.5x more according to Evercore. This reflects not only our higher GDP, but also a Faustian bargain that Pharma made around extracting marginal revenues decades ago (mentioned here). Pharma let smaller monopoly single payor systems drive down prices because they looked at it as incremental or marginal revenues after securing the largest market (the US). Unfortunately, the pricing gap is now so large that it’s no longer acceptable. It’s also a fact that the US has been subsidizing the world’s drug R&D engine, which is also likely why most of Pharma have relocated their R&D infrastructure to the US while shrinking their footprints elsewhere.
- Many innovators became addicted to US drug price increases. Over the past 20 years, Big Pharma revenue growth has become increasingly reliant on biannual US price increases, so much so the vast majority of revenue growth of the top 50 products last year was driven by price rather than volume. With industry branded drug volumes collapsing by 40% over the past six years (from 1B prescriptions in 2011 to 600M prescriptions in 2017), pricing in aggregate has been the only growth driver – either price increases of existing products, or higher pricing of new products. As I wrote in a 2016 blog on Innovators vs Exploiters, “The simple fact is the industry – including the Innovators – have gotten irresponsibly addicted to large biannual price increases for most of its products… Innovators need to take responsibility for these aggressive increases and justify them more clearly going forward.” These biannual price increases have moderated somewhat in recent years, with efforts like Brent Saunders’ price restraint pledge at Allergan. I’m very sympathetic to the claims that we need to see continued moderation in the price increases of older, existing branded drugs – unless there’s been meaningful changes to the drug’s clinical profile to justify the increase (from post-market clinical trials, for instance). And for the Exploiters who take old generic single-source products and jack up prices, in the words of Scott Gottlieb, there is no moral imperative to price gouge. It’s just not acceptable. I am hopeful with the FDA’s support of multi-source generics that these Exploiters go away.
- The mix of specialty vs primary care drugs has fundamentally changed the pharmaceutical landscape. High-priced, low-volume products are increasingly the norm. The majority of FDA approvals today now address only orphan drug populations, many of them are for ultra-orphan indications (below 10K in prevalence). This shift towards low volume products has changed the pricing paradigm, now often leading to inverse prevalence-based pricing. To me, the issue is less about the price and more about their cost effectiveness. If these new medicines truly change the lives of patients with serious orphan diseases, keeping them healthier and out of intensive hospital services or early mortality, it should be easy to justify the prices with a value-based pricing concept. With one-and-done gene therapies, this premise is even more clear. That said, the US healthcare system needs to figure out how to handle these new types of “curative” or near-curative single treatment therapies.
{kind=link}
There are many other relevant observations that could be shared about the US healthcare system and role of pharmaceuticals, but these are certainly some of the important ones.

644371744
By laying out these points though, it helps to focus attention on the things that matter for drug pricing reform: delivering value-based pricing and cost effectiveness, improving price transparency in the US system, leveraging the power generics more broadly, and reducing global pricing differentials, among other things.
Unfortunately, it’s an election year and politicians are looking for political points. It doesn’t feel good to attack the hospital in your constituency, so politicians tend not to look at healthcare services. But Pharma is always an easy target, and so the same tired drug pricing levers come up as they have for two decades: direct price negotiation (aka. price controls by a monopoly purchaser), drug importation, and international reference pricing. These aren’t the right solutions.
I’m not a policy wonk, but here are my thoughts.
A Few Drug Pricing Policy Concepts (And Recommendations for Pharma)
Encourage value-based pricing models based on cost-effective therapies – and foster more experimentation in pricing models. Pricing “what the market will bear” isn’t a viable long-term strategy in a three-tiered demand system (i.e., where the user of the product is different from the decider of product choice who is different from the payor). Instead, Pharma needs to justify much more explicitly the pricing assumptions made using value-based principles: what’s the value of the drug to the patient, caregivers, healthcare system, and society. By definition that’s hard and somewhat subjective to measure, but we need to communicate more clearly on these value aspects. The industry also needs to support objective metrics for doing health technology assessments of cost-effectiveness. Good drugs can easily justify their prices. For example, the original ICER cost effectiveness assessment of SMA gene therapy Zolgensma, the world’s most expensive drug, said it was within the “upper bounds” of the cost effectiveness framework. Of course, where the rubber meets the road on the concept of value-based pricing is where the questions arise, so understanding the exact methodologies and cost-effectiveness benchmarks is critical. Pharma needs to be at the vanguard of thought leadership in the evolution of value-based pricing models, rather than ceding intellectual ownership of this space as just a recipient of the outputs; public-private engagement to work with groups like ICER feels like a positive step forward. More experimentation on drug pricing is important, with things like pay for performance guarantees, payer volume-linked pricing (like what Alnylam has recently done), and “all you can treat” models akin to the Netflix subscription model. Legislation is needed to open the flood gates for experimentation around these topics – which right now are often suffocated by bureaucratic rules around Medicare Best Price restrictions and the like.
Facilitate greater transparency on healthcare costs and money flows – for patients and for industry players. We need to cap out of pocket costs for patients; insurance companies need to protect patients from healthcare bankruptcies and huge out of pocket expenditures – this is the essence of insurance, to protect against catastrophic outcomes. We also need to pop the “gross to net bubble” on drug prices; sending scarce healthcare resources into the pocket of middlemen in the healthcare system, where they aren’t passed on to consumers, is wrong. Legislative action needs to consider addressing both runaway patient out-of-pocket payments (an insurance issue), at the same time forcing open some transparency on where the list price rebates and discounting “savings” actually go (linking them to help reduce out of pocket costs, perhaps).
Continue expanding more generic competition, especially to establish interchangeable generic biologics. Right now over 9 out of 10 prescriptions in the US are for generic drugs, and this is a good thing. But biologics now represent 70% of the revenues of the top 15 drugs in the US. So if we are to continue to secure the benefits of commodity-priced generics, we need truly generic biologics. Given their complexity, initiatives like compulsory cell bank technology transfer at the end of a patent life (to groups like ATCC or others) to enable generic manufacturers makes sense. RA Capital’s Jessica Sagers and Peter Kolchinsky recently wrote a piece suggesting that a new regulatory body could provide oversight to create the “go generic” pathway for complex biologics; this seems like a smart concept. If the social contract is a real concept in our industry, than we need to see commodity priced generic biologic drugs in the near future. Any new drug pricing legislation needs to ensure a clear pathway here.
Reduce global price differentials for pharmaceuticals. Drug importation isn’t the answer, especially from countries with price controls (enabled by the Faustian pricing bargain described above). But this gap in pricing is becoming a trade issue. While differential pricing is commonplace in many areas of commerce, and not wrong per se, it needs to be constructed in moderation – especially for countries with similar GDP-per-capita countries. Elderly consumers often get cheaper tickets to the movies; if, by example, Britain wants to be the elderly consumer of pharmaceutical innovation, then so be it – within moderation. That decision will likely have other unintended consequences around things like R&D jobs and the like. This issue isn’t easy to solve (e.g., witness the Vertex-UK price negotiations), but has to involve some combination of higher prices from European/Asian payors and lower prices in the US. This is as much a trade issue as a legislative issue.
Promote ways to reduce the cost of capital for loss-making enterprises. In the likely future where drug pricing policy at least in part hampers risk capital, we need to figure out additional and less expensive funding sources to support emerging biotech companies, including policy measures like R&D tax credits or trading net operating losses (where buyers purchase losses for their tax benefits, thus sellers access lower cost funding). With $15-20B spent per year for R&D by private venture-backed biotechs, these policy improvements could enable billions in additional risk capital to make up for the likely equity capital outflows. Legislation should consider these efforts in particular for loss-making pharma R&D expenditures.
Those are just a few things any comprehensive drug policy legislation should consider – while emphatically reinforcing the message that the “first principle” will be protected under any future outcome – which is, again paraphrasing George Merck, that if we deliver real value to patients, the returns will follow.