



In the blink of an eye, twenty years have passed: in mid-October 2005, I joined Atlas Venture as a principal on the global life science team. We closed Fund VII a few months after I joined; and, just a few weeks ago, we closed our 11th fund since then with Opportunity Fund III. What a journey.
Like the world, biotech has changed dramatically since 2005. So has Atlas. Over the course of the first nine years after joining, we retooled ourselves from a global multi-office, multi-sector firm into a biotech-only VC based in Cambridge MA. Simplicity and focus are beautiful.
Since joining Atlas, I’ve worked with scores of biotech companies as an early stage investor and board member. I’ve also co-founded many of those along the way. I’ve had a front row seat on our emerging portfolio. It’s been an incredible ride.
Without a doubt, I love my job. The best part: the people. It’s been a privilege to work with so many wonderful people over the years – both inside of Atlas, in the portfolio, and across the industry. And, most importantly, the people we are able to help – patients. We fully embrace the double-bottom-line mantra of “doing well by doing good” at Atlas.
It’s also been hard. Venture capital is a risky business. Losses are common. I was told early in my career, perhaps tongue in cheek, that I would have to lose $100M before I’d know what I was doing. Well, I’ve gotten close to that threshold: including my unrealized positions, I’ve now lost almost $100M on paper. Thankfully, my returns outweigh those losses by a very meaningful margin.
Related to these losses is the reality of making mistakes. I’ve made plenty. But the key is to “only make original mistakes” as an early mentor told me; learn from them, try not to do them again, and share the lessons if possible.
To that end, I’ve done some reflecting on two decades at Atlas and some of the observations I’ve made along the way – insights generated by my biotech pattern recognition receptors over time. I’ve decided to share a few blogs on them.
The first, here, will be on the Science of biotech startups – we are, after all, science-first investors. I’ll follow up with one on People (talent and teams), and a final one on Business topics (BD, Boards, syndicates). There won’t be any bombshells, and I’ll disguise the innocent, but it was somewhat cathartic to think through a few of these.
So here are a handful of observations on the Science of startups from my vantage point as an early stage VC:
- Science-first opportunism beats top-down strategy for deal selection. Declaring you are going to build an Alzheimer’s company and then boiling the ocean to find the assets or platform to create a NewCo isn’t typically a route to value, despite my roots as a McKinsey consultant. I wasted time on these boiling exercises early in my career. But I quickly found that finding a nucleating asset or foundational insight in a science-first, disease-agnostic manner (via academic papers, a discussion with an entrepreneur, or an asset out-licensing list, for instance) and then building a business framework around it is much more productive. This nucleating asset can prompt aggregation of other related programs, or it can move forward as a focused asset play. Similarly, an initial platform idea may morph into an interesting albeit narrower asset-centric concept too (especially since many platforms aren’t really platforms). Opportunistically following the science may also identify other assets to bring in over time (like we did at Disc Medicine, as an example). Being business model agnostic has been important for us too: platforms/discovery engines and single asset companies create diversification in the portfolio. We shun dogmatic rules around business frameworks (“this is what a Series A should look like”) and have built an eclectic, almost artisanal, portfolio of different business models and wide-ranging scientific substrate. Starting with great science also means that we are willing to engage with a NewCo before any of the management team is in place, as we can help build the talent required to deliver on the thesis via our incubation model. All this deal-type diversity, underpinned by this science-first mindset, has rewarded us across many capital market cycles.
- Don’t believe what you read in science papers at face value. Be disciplined about academic validation and reproducibility. Lots of published findings are weak observations rather than robust discoveries. If the therapeutic hypothesis can’t be both generalizable and reproducible, it’s unlikely to survive the attrition curve of making things work inside the complexity of the human body. I’ve written on this topic many times over the years (here, here, and here), and we continue to find irreproducible science endemic. Perhaps the publish-or-perish model of an academic career leads to less stringency on the robustness of the observations that get published. This observation is why we’ve largely adopted the seed-led approach to validate novel science with “wet experiments” as a primary goal (or even as a diligence item) for many of our new startups here at Atlas. I’ve “killed” a bunch of seed-stage startups for the failure to replicate the “transformational finding” of an academic lab. Fortunately, an early kill on “small dollars” helps bend the capital-weighted risk curve of a venture portfolio in your favor.
- Don’t over-value reductionism, but also avoid phenotypic over-enthusiasm. Understanding how a drug engages its target is an important element in designing new medicines, and striving for selectivity is a valuable aspiration. However, taking an overly reductionist view of molecular drug targets is fraught with error as the precision of selectivity is often wrong in a world of promiscuous interactions. Reality is most (small molecule) drugs when dosed in the human body engage multiple targets, in part due to the massive concentration differences across peak to trough on a PK curve. But the converse of being overly-reductionist is even more true: phenotypic effects with unknown targets make for challenging drug discovery. I frequently recall one of Phil Needleman’s rules: phenomenology is different than pharmacology. The former often involves things like “cellular homeostasis”, “oxidation states”, “RNA expression patterns” or other fuzzy cellular observations. The latter (pharmacology) is about truly understanding PK/PD relationships around specific molecular mechanisms. For discoveries from phenotypic screens, target deconvolution is key; but even with all the great tools today, it remains hard to do. In the right settings, it’s ok to take on trying to “find the target” in the context of an investment – and we’ve done this a number of times, including recently. But if you can avoid it and embrace the reductionist view (sometimes illusion) of target identification/validation, it makes the downstream job easier – both for R&D reasons (like lead optimization and candidate selection) and for business reasons (like funding the company!). Investors and Pharma partners want to know you know the target, even if everyone sort of winks while they say it.
- Rare disease drug development isn’t as “easy” as it seems on paper. Orphan drugs have generally been an exciting area of discovery for biotech over the past couple decades, and over 50% of recent FDA approvals are for “rare” diseases. But startups often approach these opportunities under the misguided notion that rare means less expensive and shorter timelines. That can certainly be the case, but only if there are solid natural history datasets and a fulsome understanding of the disease course and presentation. And in cases like that, there are often predicate standard of care drugs that require comparative trials, making them longer and more expensive. Doing a placebo-controlled trial (vs open label) in many rare diseases is really quite challenging today (often untenable from a financing perspective, which I’ve learned first-hand). It’s true that the size of the Phase 3 program (measured in number of patients enrolled) is much smaller than for larger disease settings, but there are lots of other costs in rare settings (including random things like flying in hard-to-find patients for gene therapy procedures, as one example). Further, because many rare diseases don’t have a comprehensive deep clinical understanding, the “unknown unknowns” can bite you; for example, knowing what the background rate of pulmonary embolisms is in Prader-Willi Syndrome, or suicidality in Huntington’s, or what a brain MRI should look like over the course of a rare neurodegenerative disease… all become important in the clinic with implications for powering, safety interpretation, and others. I’ve seen experienced all of those, and more, in our rare disease portfolio.
- The single most important value creation activity in biotech is excellent clinical trial execution. Rapid trial enrollment, with the right inclusion/exclusions, with robust and consistently-measured endpoints, and delivered on time (all the way to database lock and top line data) – these are the things that unlock real value from the Science in startups. After years in discovery, the clinic makes or breaks everything, so never cut corners or shortchange on an important early clinical trial. It’s oddly funny that the single most important event for an emerging biotech is often the one that is largely outsourced to clinical CROs. We lease lab space, do all these in vitro experiments on our own benches, use expensive machines to augment our discovery DMTA cycles, build vivariums for animal work… but then outsource all of our clinical execution to a CRO? Clearly not the right answer. Partnering with a CRO is almost always required in light of a small biotech’s organizational limitations, but never delegate the important details to a CRO, or assume things are going to go fine. For early patient trials, in particular, a startup’s Chief Medical Officer should be signing off on every patient enrolled – understanding who is being put on the drug and adjudicating questionable participants. Sending team members to be onsite with both the CRO’s field team and the clinical investigators during the initial doses (and beyond) is smart. Hiring additional clinical research folks is often well worth it. We’ve had patients put on trials that shouldn’t been enrolled, or where the trial participant did stupid things (like running marathons right before blood work), or even where trial sites were fraudulently making up data to get paid. Most CMOs with grey hair have tons of stories like these and more. In addition, don’t skimp on the funding of the trial: when you can afford it, buy more power with a few more patients… rarely a regret. Bottom line is you can’t be all over the details too much in clinical development.
- Novelty is great, but only when it’s unlocking something truly valuable to patients. Taking on novel biology or novel modality risk is only worth doing if it delivers compelling clinical performance. Cool science is not enough. A new first-in-class drug against a genetically-validated target that only performs as well as generic drugs from older classes just isn’t interesting (or shouldn’t be) – despite how sexy the science is. That’s novelty for novelty, rather than novelty for patient value. Further, taking a novel modality and derisking it with a “known validated target” with intense competition just isn’t very compelling (like the Ab-like scaffolds in the mid-2000s all chasing TNF and CD20) – unless you truly believe it will differentiate as a best-in-class asset. I firmly believe new modalities or novel complex therapies need to do truly new things, like making the previously undruggable become a viable target addressing an important medical need.
- Be skeptical, as most things fail, but embrace “a permission to believe”. There are 100s of reasons why a drug could fail, so much so that it’s easy to become cynical in this business. Saying “no” during diligence is the right answer in the majority of cases over a long enough time interval, given attrition rates. But asking what is really required to say “yes” – that’s the better question. Focusing on the few scenarios for where it could actually “work” as a drug is often important. Obviously, being irrational about its success isn’t helpful, but thoughtfully understanding what you’d need to see at every step of the drug R&D process is key. What are the lead characteristics or DC criteria (linked to a Target Product Profile grounded in commercial or competitive reality) that give us confidence in moving forward to lead optimization or Phase 1, respectively. What is the clinical profile we expect to see in early studies. Defining these frameworks upfront, with go/no-go scenarios done a priori, can greatly aid in the decision rubric when the time comes – and help keep everyone honest if a drug will make it or not. Confirmation bias and group think often overwhelms healthy skepticism, especially if you don’t articulate the rules of the game beforehand. Being disciplined is the key. But there’s a positive side to the discipline too: thinking about the scenarios beforehand means that if the data starts to reveal itself in a truly positive way, it helps teams be ready to accelerate.
- Understand the real risk you are underwriting and the value of discharging it. Science risk is only one of them, and often it’s not the most expensive to discharge; non-technical risks like differentiation risk, financial risk, execution risk, team risk, regulatory risk, or even geopolitical risk are often important. My friend Mike Gilman blogged beautifully on this point years ago, and it’s all still salient today. Competitive risk is often a late stage and expensive risk to discharge (in head-to-head Phase 2b/3 studies) relative to a novel biology risk (often in a small Phase 1b patient study). Differentiation like dosing convenience can often be derisked early with PK data (e.g., this mAb has twice yearly dosing vs a weekly SoC), but proving better efficacy (like deeper response rates) often requires bigger, longer trials. Having to run a big placebo-controlled phase 3 to find out if you’re comparable to a standard of care has a big dollar-weighted risk profile. One real clinical execution risk, often overlooked, is the veracity of the primary endpoint itself: taking a novel unproven metric as your primary can be really risky, and we’ve been burnt on the “cool” novel endpoint in the past (e.g., as I learned using Sitzmarks radiopaque markers as the endpoint for IBS motility circa 2008). And don’t forget about CMC risk, an often overlooked and yet hugely critical element in biotech; a 30-step synthesis that takes 6-9 months to make enough material also adds to the financing risk. The reality is we always are taking a healthy dose of risk in biotech – but accept the risk burden only when you really have to (in order to drive value), and not in other domains of the plan, where it feels like excess or incremental risk without the upside. It’s also key as an investor (or CEO) to make sure you know what risk you are expecting to discharge with the capital (or time) you are investing, and the likely value accretion in doing so.
- Seek the scientific truth, not just “making money”. I firmly believe that in the long run doing quality science and being data-driven unlocks value. If there are questions that can be answered that help you undercover whether you have a real drug or not, then answer them. Do the experiments that tell you if you have a false positive (a drug candidate that is actually not going to make it) – before you put patients at risk. Every once in a while I’ll hear things like “we don’t want to know that answer” – with the fear that the data could kill their potential drug before it gets tested clinically or monetized in a deal. This is almost never the right call – for companies and investors in the long run, and especially for the patients who volunteer in our studies. Do good science, leverage all the tools you can to learn about your drug program, and in the long run value will most likely accrue to you.
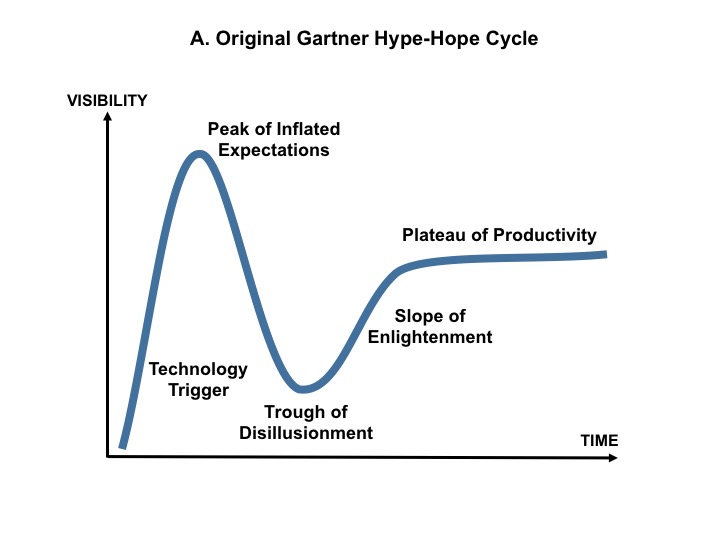
- Innovation and optimism are tightly interconnected – and have been ever present in biotech. In every period over the past twenty years, I’ve felt innovation couldn’t be more exciting – and that it was always accelerating. Back in 2005, the Human Genome had only been sequenced a few years before, with ultra-high-throughput sequencing opening up the analysis of genetic variants, and technologies like RNAi and SBDD were shiny new toys with enormous promise. A few years later, breakthroughs in gene and cell therapy (AAV, LV, CART) in both cancer and rare disease reignited those areas. Then the I/O revolution and CRISPR. Today its degraders, bi/tri-specifics, ADCs, RLT, base editing, and so much more. But, in every period, it always seems like we’re the cusp on great advances, with wonderful new medicines just out in front of us, and are optimistic about the impact of science. Today is always more exciting than yesterday, it seems. Of course, novel discoveries take years or even decades to turn into products, and each new concept travels thru the ups and downs of the Gartner hype-hope innovation cycle. But through all this the flame of eternal optimism just keeps burning – part of what makes this innovation business so exciting.
{kind=link}
This optimistic note is a great one to end on. Plenty of other observations about R&D and science in biotech that I could have highlighted, but those are a good hit list.
Next up will be People and talent!